Patient Outcome
Restoring Health, Comfort, and Aesthetics by Eliminating Diseased Teeth
Phil had battled advanced periodontal disease and failing teeth for years.

Before
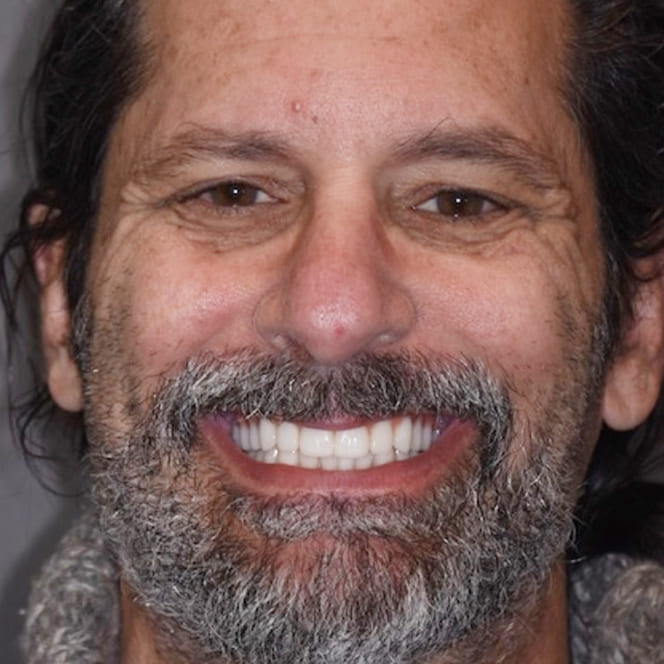
After
Patient
Phil
Surgeon
Dr. John E. Lofthus
Recovery
8-12 months
"For years I dreaded going to the dentist because the news was always bad. Now I have a smile that works, feels natural, and does not cause me pain. I feel like I got a second chance."
Phil had been fighting advanced periodontal disease for over fifteen years by the time he came in for his first consultation. Multiple rounds of scaling, root planing, and antibiotic therapy had slowed the progression without stopping it. Several teeth had become mobile, chronic infection had made eating painful, and the situation had grown socially difficult to manage.
Three teeth had already been extracted before his referral. His general dentist had deemed several others unrestorable. Phil didn't need another maintenance cycle — he needed a definitive plan that would eliminate the disease, restore function, and give him a stable, long-term result he could rely on.
Initial Condition & Severity
Phil presented with generalized severe chronic periodontitis. Radiographic evaluation showed bone loss exceeding 60 percent around multiple teeth in both arches. Several teeth had Grade III mobility and purulent drainage on probing at multiple sites.
Many of the remaining teeth were variously compromised. Some had furcation involvement that ruled out successful retention; others had root fractures that had gone undetected until imaging. The overall bacterial burden was high, and the chronic inflammatory state had implications for his general health beyond his mouth.
Phil's primary complaints were pain when eating, a persistent bad taste, and the embarrassment of teeth that were visibly deteriorating. He wanted something definitive — not another temporary fix.
Why Saving the Teeth Was Not Viable
There is often a reasonable desire to preserve natural teeth wherever possible. In Phil's case, the clinical reality made that approach counterproductive.
- Teeth with Grade III mobility and advanced bone loss cannot be predictably stabilized, and keeping them in place maintains a chronic source of bacterial infection.
- Molar teeth with through-and-through furcation involvement carry a poor long-term prognosis even after surgical intervention.
- Sustained periodontal infection has documented systemic health implications, including associations with cardiovascular disease and metabolic conditions.
- Removing hopeless teeth strategically allowed implants to be placed in positions dictated by ideal biomechanics, rather than constrained by compromised anatomy.
Treatment Plan & Staged Approach
A phased treatment plan was developed starting with strategic extraction of all teeth identified as hopeless, followed by guided bone regeneration at sites with significant defects, and concluding with implant placement and final prosthetic restoration.
Phil would be in an immediate provisional denture throughout the healing phases — never without teeth. The provisional also functioned as an early test of aesthetics and function, providing a template for the final prosthesis design before any permanent work was committed to.
Eight implants were planned across both arches, positioned to support fixed hybrid prostheses. The goal was full-arch function without the instability or maintenance burden of conventional removable dentures.
Case Progression & Key Milestones
Phase one involved extraction of eleven teeth with simultaneous bone grafting at the most deficient sites. Immediate provisional prostheses were delivered the same day, so Phil left the office with a functional smile.
Four months later, cone-beam imaging confirmed adequate bone regeneration at the grafted locations. Implant placement was staged across two surgical visits two weeks apart to keep the scope of each appointment manageable.
Following a four-month integration period, all implants demonstrated excellent stability. The final prostheses were fabricated using a digital workflow that verified fit and occlusion precisely before delivery.
The full timeline from initial extractions to final restorations was approximately eleven months, with functional provisional prostheses at every stage.
Outcome
Phil's transformation was dramatic. Chronic infection, persistent pain, and progressive tooth loss were replaced with stable, functional, implant-supported dentition that looked and felt natural.
The fixed prostheses allowed him to eat foods he had avoided for years. The bad taste associated with active infection was gone. His speech improved, and he reported feeling like he had recovered a decade of quality of life.
At his one-year follow-up, all implants remained stable, peri-implant tissues were healthy, and Phil had maintained excellent home care. He described the decision to commit to a comprehensive plan — rather than continuing to patch individual failing teeth — as the best health decision he had ever made.
Clinical Notes
This case demonstrates that strategic extraction combined with implant-supported rehabilitation can offer a superior long-term outcome compared to repeated attempts to salvage teeth with a hopeless prognosis.
The key to success in full-arch implant rehabilitation is meticulous preoperative planning, including CBCT-guided implant positioning, adequate bone volume assessment, and thoughtful prosthetic design before any surgery begins.
- Guided bone regeneration at extraction sites with severe defects was essential for creating adequate implant receptor sites.
- Immediate provisional prostheses maintained patient function and aesthetics throughout the healing and integration phases.
- Digital prosthetic workflow provided superior fit accuracy and allowed precise verification of occlusion before final delivery.
Your Story Starts Here
Ready to See What's Possible?
Request a consultation and let our specialists evaluate your situation. Clear options, honest answers, no pressure.